All published articles of this journal are available on ScienceDirect.

Experimental and Finite Element Investigations on the Biomechanical Consequences of Meniscectomies in the Knee Joint: A Narrative Review
Abstract
Background:
The knowledge of the complex biomechanical behaviour of the meniscectomised knee joints is of paramount importance in various clinical situations. A combined review of experimental and finite element analysis studies examining the consequences of meniscectomies on the biomechanics of the knee joint has not been reported in the literature. Therefore, this paper presents a combined review of experimental and finite element analysis studies on the biomechanical consequences of medial and lateral meniscectomies in the knee joint.
Methods:
Experimental and FEA investigations on the association between meniscectomies and the biomechanical response of the knee joint are reviewed. The effects of partial and total meniscectomies in the medial and lateral compartments are included in this paper.
Results:
Subtotal/total medial meniscectomies cause a significant decrease in the contact area and a substantial increase in the contact stress in comparison with that in an intact knee joint. This could give rise to severe degeneration of the cartilage surface. Partial medial meniscectomy causes a modest reduction in the contact area associated with a moderate increase in contact stress. The resection of both leaflets of the meniscus results in a substantial increase in the contact pressure and a significant reduction in contact area compared with inferior leaflet resection.
Conclusion:
This review recommends partial medial meniscectomy over subtotal/ total medial meniscectomy. It also suggests performing resection of the inferior leaflet rather than resection of both the leaflets. Finally, some recommendations for future work are suggested to predict the realistic biomechanical behaviour of meniscectomised knee joints.
1. INTRODUCTION
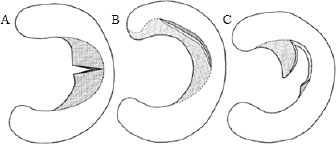
The menisci are significant structures that transmit the load, absorb the shocks, and stabilize and lubricate the knee joint [1]. They are semilunar fibrocartilaginous structures that are situated between the load-bearing joint surfaces of the femur and tibia in the knee [2]. The wedge shape of the meniscus enables it to facilitate the uniform distribution of load [3] and provide stability to the knee joint. Meniscal injuries typically occur by trauma or through gradual degeneration. In young subjects, they occur as a consequence of high knee joint forces and moments while performing sports-related activities [4]. Injury to the meniscus (meniscal tear) changes the load transfer, giving rise to elevated contact pressure (CP) and lesser contact area (CA) in the knee joint [5]. Tears in the outer periphery of the meniscus have a better possibility of healing because of good blood supply [6]. The supply of blood in the inner two-thirds of the meniscus is less, which results in the lesser healing ability of the tear in this region. Further, the knee may be locked when torn pieces of the meniscus get into space within the joint. Partial meniscectomy is a type of meniscectomy that excises only the loose and fragile portion of the torn meniscus [7] and preserves a steady and balanced peripheral rim of the healthy meniscus. Fig. (1) shows the partial meniscectomies for treating radial, longitudinal and flap tears. Subtotal meniscectomy is the resection of posterior, middle and anterior portions leaving behind a small peripheral rim [8]. Total meniscectomy is the resection of the whole meniscus and is carried out under circumstances where the damage in the meniscus is beyond repair or partial resection. It causes severe degenerative changes in the cartilage resulting in osteoarthritis [9].
Experimental studies have been conducted to predict the biomechanical behaviour of the knee joint following different types of meniscectomies. They include techniques such as arthrography [11, 12], load-deflection studies [13, 14], intra-articular casting [15, 16], photoelastic studies [17], and intra-articular pressure measurements [18-20]. In addition to experimental studies, finite element analysis (FEA) studies have also been used to investigate the changes in biomechanics after meniscectomies.
Several researchers have investigated the impact of meniscectomies on the biomechanics of the knee joint. For instance, Lau et al. [21] reviewed experimental studies examining the biomechanical effects of meniscectomies in the knee joint. It was found that meniscectomy led to an increase in CP along with a decrease in CA. However, this paper reviewed only a few experimental studies exploring the effects of meniscectomies on the contact parameters of the knee joint. Furthermore, Pena et al. [22] presented a review of FEA studies examining the impact of meniscectomies on the biomechanics of the knee joint. In addition, Kazemi et al. [23] reviewed finite element (FE) models exploring the changes in the functioning of the knee joint following meniscectomies. Furthermore, Trad et al. [24] provided a review on the application of FEA studies in the investigation of the biomechanical effects of ligament injury and meniscectomy in the knee joint. In addition, Cooper et al. [25] presented a review of the current challenges in the FE modeling of the knee joint and the investigation of validation strategies. All these reviews considered only a few FEA studies exploring the consequences of meniscectomies on knee biomechanics. However, to the best of the authors’ knowledge, there is no reported combined review on experimental and FEA studies that have examined the changes in biomechanics after meniscectomies. Hence, this paper presents the review of experimental and FEA studies carried out to investigate the effects of medial and lateral meniscectomies on the biomechanics of the knee joint.
2. REVIEW OF EXPERIMENTAL STUDIES
The experimental setup consists of a test rig, which is used to mount the cadaveric knees and apply the loads at different flexion angles. The CA can be measured using the casting method, X-ray and pressure transducers, whereas pressure can be measured using pressure-sensitive sheets and pressure transducer. This section discusses the effects of medial and lateral meniscectomies on knee biomechanics.
2.1. Medial Meniscectomy
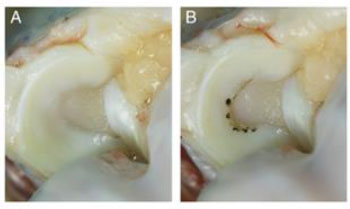
Numerous experimental studies have investigated the effect of partial medial meniscectomies on the biomechanics of the knee joint. For example, an experimental study demonstrated a decrease in CA of 10% relative to that of the intact joint after 33% partial meniscectomy [26], while another study [27] found a corresponding decrease in CA of 13%. In a similar study, it was reported that CA decreased by 20% after 50% partial meniscectomy [28]. It could be observed that the findings were in agreement with each other. Furthermore, experimental studies showed an increase in the contact stress of 65% after 33% partial meniscectomy in the inner one-third of the meniscus [26], while it was 35% after 50% partial meniscectomy of the posterior horn of the meniscus [28]. The difference in the regions of meniscectomy could be the reason for the disparity in the results. In addition, studies reported an increase in CP of 45% [29], 58% [30] and 61% [31] after partial medial meniscectomy (Fig. 2). It could be observed that these findings were comparable with each other. Together, these studies manifested that partial meniscectomy causes a moderate reduction in CA (range of 10-20%), a significant increase in contact stress (range of 35-65%), and a considerable increase in CP (range of 45-61%) compared with the intact knee. Moreover, it was found that partial medial meniscectomy resulted in moderate degenerative changes in the cartilage [32-34].
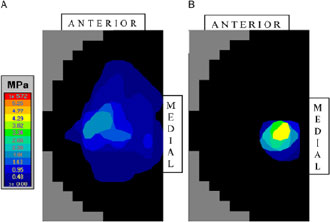
While the discussions above focused on the effects of partial medial meniscectomies, it may also be important to investigate the effects of total medial meniscectomies on biomechanics. Few experimental studies reported a reduction in CA of 46% [27] and 49% [28] after total medial meniscectomies at 00 flexion, while other studies reported a corresponding reduction of 55% [35], 30% [36] and 40% [37] at 300 flexion (Fig. 3). However, some of the studies obtained a reduction in CA of 70% [18] and 80% [38] at flexion angles of 600 and 500, respectively. Furthermore, an experimental study showed a rise in contact stress of 235% [26], while another study demonstrated a rise of 136% [28]. The variation in the findings could be due to the difference in the flexion angle, experimental methods and anatomy of the specimens. In addition, studies reported that total medial meniscectomy caused an increase in CP of 48% [36] and 70% [37]. It could be observed that these findings were comparable with each other. Together, these experimental studies revealed that total medial meniscectomy results in a substantial reduction in CA (range of 36-80%), a significant increase in contact stress (range of 136-235%) and a considerable increase in CP (range of 48-70%) in comparison with the intact knee. Moreover, it was observed that total medial meniscectomy led to severe degenerative changes in the cartilage [9, 32-34].
Several experimental studies have reported the effects of medial meniscectomies (excision of leaflets of medial meniscus) used to treat horizontal cleavage tears (HCT) on the biomechanical parameters of the knee joint. In one study, it was observed that CP increased by 34% after the resection of inferior and superior leaflets in comparison with that in the intact knee [39]. In another study, it was reported that CP increased by 36% after inferior leaflet resection whereas it increased by 79% after resection of inferior and superior leaflets [40]. Furthermore, it was found that CP increased by 24% after inferior leaflet resection whereas it increased by 51% after resection of inferior and superior leaflets [41]. The disparity in these findings could be due to the difference in experimental methods and conditions. It could be observed that there is a greater increase in CP in the case of resection of both leaflets compared with that in the case of inferior leaflet resection. This is because of the larger reduction of collagen fibre bundles in the meniscus corresponding to the resection of both leaflets [42]. Together, these studies demonstrate that resection of both leaflets results in a greater increase in CP compared with inferior leaflet resection. Hence, it would be advisable to perform resection of an inferior leaflet rather than resection of both leaflets.
2.2. Lateral Meniscectomy
Several researchers have explored the impact of partial lateral meniscectomy on knee biomechanics. It was found that partial lateral meniscectomy resulted in a reduction in CA of 57% [5] and 44% [43]. It could be observed that the results were in agreement with each other. Further, partial lateral meniscectomy caused a rise in CP of 36% [5] and 42% [43]. However, another study [44] reported an increase in CP of 12%. This may be because of the smaller magnitude of load considered in this study compared with other studies [5, 43]. Together, these experimental studies revealed that partial lateral meniscectomies cause significant changes in CA and CP in comparison with that in the intact knee.
In addition to exploring the impact of partial lateral meniscectomy, some researchers have also explored the relationship between total lateral meniscectomy and the biomechanical response of the knee joint. One study found a decrease in CA of 65% in the tibial cartilage in comparison with that in the intact knee [45], while another study showed a corresponding decrease of 33% [27]. The disparity in these results could be because of the difference in experimental methods and loading conditions. Furthermore, an experimental study observed an increase in CP of 100% after total lateral meniscectomy [45]. Therefore, these findings confirmed that total lateral meniscectomy results in a considerable reduction in CA along with a significant increase in CP.
Only one study has investigated the consequences of meniscectomy (resection of leaflets) to treat HCT on the biomechanical parameters of the knee joint. A study by Koh et al. [46] investigated the effects of inferior and superior leaflet resection of the lateral meniscus on contact mechanics of knee joint. It was found that the peak pressure increased by 27% after the resection of the inferior leaflet, whereas it increased by 39% after resection of inferior and superior leaflets, as compared with the intact knee joint. Also, it was found that CA decreased by 35% after resection of the inferior leaflet whereas it decreased by 50% after resection of inferior and superior leaflets, as compared with that of the intact knee joint [46]. Hence, it could be established that resection of both leaflets results in a greater increase in CP and greater reduction in CA compared with inferior leaflet resection. Therefore, it would be advisable to perform resection of an inferior leaflet rather than resection of both leaflets. The summary of the literature related to experimental studies is depicted in Table 1.
3. REVIEW OF FINITE ELEMENT ANALYSIS STUDIES
Experimental studies can only measure stresses normal to the surface of the joint. However, FEA has the advantage of measuring stresses not just at the surface but also across the depth and in all tensor directions. FEA helps in the study of stress distribution [47] in various parts of the knee joint. In addition, 3D FE models have proved to be versatile in capturing the realistic biomechanical behaviour of the meniscectomised knee joints. However, FEA studies could give precise results after meniscectomies provided exact geometry, complex material behaviour, actual loads and boundary conditions are taken into account.
| Study/Ref | Year | Age (Yrs) | Number of Subjects | Condition | Method | Key Findings |
|---|---|---|---|---|---|---|
| Baratz et al. [26] | 1986 | NA | 07 | Meniscectomy to treat bucket handle tear in MM (inner one-third) | 1800 N, pressure-sensitive film | Decrease in CA by 10% and 75% after partial and total meniscectomy, increase in contact stress by 65% and 235% after partial and total meniscectomy |
| Ihn et al. [27] | 1993 | 17-56 | 05 | Medial meniscectomy | 120 kg, standard film pressure chart and polar planimeter | Decrease in CA from 11.2-9.7 cm2 (13%),11.2 - 6.1 cm2 (46%) after partial and total medial meniscectomies, respectively, 10.1-6.8 cm2 (33%) after total lateral meniscectomy |
| Lee et al. [28] | 2006 | 53 (38-61) | 12 | Medial meniscectomy in the red-white and red-red regions | 1800 N, Tekscan pressure sensor | decrease in CA of 20% and 49% after 50% and total meniscectomies, respectively, increase in contact stress of 35% and 136% after 50% and total meniscectomies, respectively |
| Bedi et al. [31] | 2010 | 61.25 (57-68) | 8 | Meniscectomy to treat a radial tear in MM (junction between the body and posterior horn) | Knee joint simulator-physiological load at 14% (2100 N) and 45% of the gait cycle (approx. 2000 N), Tekscan pressure sensor | Partial meniscectomy caused a rise in CP of 45% |
| Pozzi et al. [30] | 2010 | NA | 8 | medial meniscectomy | 300 N, Tekscan pressure sensor | increase in peak CP of 58% after 75% meniscectomy |
| Zhang et al. [32] | 2015 | 64 (63-65) | 6 | Meniscectomy to treat 75% radial tear in MM (posterior horn) | 1000 N, Tekscan pressure sensor | peak CP increased from 0.9±0.1 MPa to 1.45±0.2 MPa (61%) after 75% meniscectomy |
| Lewinski et al. [35] | 2006 | NA | 12 | medial meniscectomy | 500 N, Tekscan pressure sensor | reduction in the CA of about 55% |
| Muriuki et al. [36] | 2011 | 53.6 (46-72) | 11 | Meniscectomy to treat a radial tear in MM (body, 66% tear) | 1000 N, pressure-sensitive film | Total medial meniscectomy resulted in a 36% reduction in medial CA and a 48% increase in peak CP |
| Seitz et al. [37] | 2012 | 44.5 (29-60) | 10 | Meniscectomy to treat a radial tear in MM | 1000 N, Tekscan pressuresensor | total medial meniscectomy caused a 40% decrease in the CA and a 70% increase in CP |
| Ahmed and Burke [18] | 1983 | 61 (49-76) | 18 | Total medial meniscectomy | 1335 N, micro indentation transducer | Reduction in CA of 70% after total medial meniscectomy |
| Cottrell et al. [38] | 2008 | NA | 06 | Total medial meniscectomy | Knee joint simulator, Tekscan pressure sensor | 80% reduction in CA after total medial meniscectomy |
| Brown et al. [39] | 2015 | 80 (55-86) | 12 | Resection to treat HCT in MM (posterior horn- 1.5 cm width) | 1800 N, Tekscan pressure sensor | CP increased by 34% after the resection of inferior and superior leaflets |
| Koh et al. [40] | 2016 | 52 (22-73) | 12 | Resection to treat HCT in MM | 800 N, Tekscan pressure sensor | CP increased by 36% after inferior leaflet resection whereas it increased by 79% after resection of inferior and superior leaflets |
| Haemer et al. [41] | 2006 | NA | 16 | Resection to treat HCT in MM | 1023 N, Tekscan pressure sensor | CP increased by 24% after inferior leaflet resection whereas it increased by 51% after resection of inferior and superior leaflets |
| Bedi et al. [5] | 2012 | NA | 6 | Meniscectomy to treat a radial tear in LM | Knee joint simulator-physiological load at 14% (2100 N) and 45% of the gait cycle (approx. 2000 N), Tekscan pressure sensor | 36% increase in CP and 57% reduction in CA after partial lateral meniscectomy |
| Prince et al. [43] | 2013 | 49.1(44.1-54.1) | 10 | Meniscectomy to treat a radial tear in LM | 1000 N, Tekscan pressure sensor | 42% increase in CP and 44% reduction in CA after partial lateral meniscectomy |
| Goyal et al. [44] | 2014 | 55(43-67) | 10 | Meniscectomy to treat a longitudinal tear in LM (posterior horn) | 550 N, pressure-sensitive film | Lateral meniscectomy resulted in a 12% increase in peak CP |
| Ode et al. [45] | 2012 | 65(50-82) | 5 | Meniscectomy to treat a radial tear in LM | load of 800 N, Tekscan pressure sensor | 100% increase in CP and 65% reduction in CA after total lateral meniscectomy |
| Koh et al. [46] | 2018 | (54-65) | 11 | Resection to treat HCT in LM (50% tear) | load of 800 N at flexion angles of 00 and 600, Tekscan pressure sensor | CP increased by 27% after inferior leaflet resection whereas it increased by 39% after resection of inferior and superior leaflets, CA reduced by 35% after inferior leaflet resection whereas it reduced by 50% after resection of inferior and superior leaflets |
3.1. Medial Meniscectomy
Many FEA studies have focussed on the changes in the biomechanics of knee joint after partial medial meniscectomy. FEA studies demonstrated an increase in maximum compressive stress (MCS) of 32% [47], 55% [48], 43% [49], 28% [50] and 78% [51] after partial medial meniscectomy in the tibial cartilage in comparison with that in a healthy knee joint. In another study [52], it was observed that partial medial meniscectomy caused an increase in the Von Mises stress of 72% in the tibial cartilage. Furthermore, it was found that partial medial meniscectomy led to an increase in CP of 14% and a reduction in CA of 6% in the cartilage relative to that of the intact knee joint [53]. In addition, it was observed that partial medial meniscectomy caused a rise in the maximum shear stress of 98% [54]. Together, these studies demonstrated that partial medial meniscectomy gives rise to a significant increase in MCS (range of 28-78%), maximum shear stress and CP and a modest reduction in CA in the cartilages compared with that in a healthy knee joint.
Few researchers have discussed the effects of subtotal medial meniscectomies on the biomechanical response of the knee joint. For instance, an FEA study reported a rise in the CP of 20% and a reduction in CA of 28% in the medial tibial cartilage relative to that in an intact knee after subtotal meniscectomy [53]. Also, the rise in CP on MM was observed to be 70%. Another FEA study by Devaraj et al. [55] found that subtotal meniscectomy caused an increase in MCS (mean±95% CI) of 21.53±8.84%, rise in CP of 22.25±10.38% and a reduction in CA of 17.6±4.6%. Also, the rise in CP on MM was observed to be 82.13±38.97%. Together, these studies demonstrated that subtotal medial meniscectomy causes a significant reduction in CA (range of 18-28%), a considerable rise in MCS, a remarkable increase in CP (range of 20-22%) in the medial tibial cartilage along with a rise in CP on MM (range of 70-82%). This could be attributed to the loss of hoop tension in the meniscus after the removal of the larger portion of the meniscus during SM [56]. Moreover, it was observed that subtotal medial meniscectomy led to severe degenerative changes in the remaining meniscal tissue [48, 57].
The relationship between total medial meniscectomy and the biomechanical response of the knee joint has been demonstrated by several FEA studies. For instance, an FEA study found an increase in MCS of 302% and a decrease in CA of 45% in the tibial cartilage after total meniscectomy [47] in comparison with that in the intact knee joint. Furthermore, a rise in CP of 26% and a decrease in CA of 26% in the tibial cartilage were observed after total meniscectomy [53]. Another study [58] reported an increase in CP of 48% after a total medial meniscectomy. In a similar study, an increase in the maximum shear stress of 177% was found after a total medial meniscectomy [54]. Together, these studies manifested that total medial meniscectomy causes a substantial reduction in CA along with a considerable rise in MCS, CP and maximum shear stress.
3.2. Lateral Meniscectomy
Although several studies have discussed the effects of partial medial meniscectomies on knee biomechanics, only a few studies have reported the effects of partial lateral meniscectomies. For example, in one study, it was found that partial lateral meniscectomy caused an increase in the maximum shear stress of 415% in the cartilage [54]. In another study, partial lateral meniscectomy caused an increase in MCS of 44% and CP of 50% [4]. Together, these results indicated that partial lateral meniscectomy gives rise to a significant increase in the maximum shear stress, CP, and MCS in the cartilage.
Furthermore, it was demonstrated that total lateral meniscectomy caused an increase in the maximum shear stress of 687% in the tibial cartilage. Also, the increase in maximum shear stress after lateral meniscectomy was significantly higher when compared with that after medial meniscectomy (177%) [54]. This could be because of the difference in congruity between the surfaces of femoral and tibial condyles in the medial and lateral compartments of the knee joint. Thus, it can be concluded that total lateral meniscectomy causes a substantial rise in the maximum shear stress in the tibial cartilage. The summary of the literature related to FEA studies is depicted in Table 2 [47-59].
4. CORRELATION BETWEEN FINITE ELEMENT ANALYSIS (FEA) AND EXPERIMENTAL STUDIES
FEA is a powerful technique that has been frequently used to solve biomechanical problems. However, it is necessary to validate the findings against experimental results to check the accuracy of the solution. The correlation between FEA and experimental studies was as follows:
| Authors/Ref | Year | Condition | Boundary Conditions | Key Findings | ||
|---|---|---|---|---|---|---|
| Pena et al. [47] | 2005 | Medial meniscectomy | 1150 N, full extension, constrained varus-valgus and flexion-extension rotations of the femur, fixed lower surface of the tibia | MCS increased from 2.55-3.36 MPa (32%) after partial medial meniscectomy, MCS increased from 1.2-4.83 MPa (302%) and CA reduced by 45% after total medial meniscectomy | ||
| Zielinska and Donahue [48] | 2006 | Medial meniscectomy | 1200 N, full extension, proximal surface of femur was fixed, rotation of tibia was fixed | 55% increase in MCS after medial meniscectomy | ||
| Dong et al. [49] | 2014 | Resection to treat a longitudinal tear in MM | 1150 N, full extension, constrained varus-valgus and flexion-extension rotations of the femur, fixed lower surface of tibia and fibula | Partial Meniscectomy (~30%) caused an increase in CP from 2.75 -3.92 MPa (43%) in the tibial cartilage. | ||
| Zhang et al. [50] | 2019 | Meniscectomy to treat Radial Tear (60%) in MM | static stance - 1150 N, fixed lower surfaces of tibia and fibula, all degrees of freedom were unconstrained for femur | MCS increased from 5.02 to 6.41 MPa (28%) after medial meniscectomy | ||
| Li et al. [51] | 2019 | Resection to treat Big oblique tear in MM | 1150 N, balanced standing posture, tibia and fibula fixed, translation and rotational degrees of freedom unconstrained | MCS increased from 3.97 to 7.1 MPa (78%) after medial meniscectomy | ||
| Yang et al. [52] | 2022 | Resection to treat posterior root tear in MM | Axial force of 1000 N, the tibia was fixed, and the femur - free to translate in the axial and free to rotate about internal and external axes. | Von mises stress increased from 3.97 to 7.1 MPa (78%) after medial meniscectomy | ||
| Bae et al. [53] | 2012 | Medial meniscectomy | Single leg stance under full extension -570 N on the sacrum, x-direction displacements of the sacrum and coxal bones were fixed, distal surfaces of tibia and fibula were fixed | Increase in CP of 14% and reduction in CA of 6% after a partial meniscectomy, a rise in the CP of 20% and a reduction in CA of 28% in the medial tibial cartilage, a rise in CP on MM of 70% after subtotal meniscectomy [51]. Increase in CP of 26% and reduction in CA of 26% after total meniscectomy | ||
| Devaraj et al. [55] | 2021 | Medial meniscectomy | 1150 N, full extension, constrained varus-valgus and flexion-extension rotations of the femur, fixed lower surface of tibia and fibula | subtotal meniscectomy gave rise to an increase in MCS (mean±95% CI) of 21.53±8.84%, rise in CP of 22.25±10.38% and reduction in CA of 17.6±4.6% in the cartilage, rise in CP of 82% on MM | ||
| Wang et al. [58] | 2022 | Total medial meniscectomy | Load corresponding to single stance during the gait cycle | Total meniscectomy led to an increase in the CP of 48% in the tibial cartilage | ||
| Pena et al. [52] | 2006 | Lateral and Medial meniscectomy | 1150 N, full extension, constrained varus-valgus and flexion-extension rotations of the femur, fixed lower surface of tibia | Increase in maximum shear stress of 98% and 177% after partial and total medial meniscectomies, respectively, Increase in maximum shear stress of 415% and 687% after partial and total lateral meniscectomies, respectively | ||
| Mononen et al. [4] | 2013 | Radial Tear (66%) in LM | Gait cycle data was applied on the reference point, the bottom surface of tibial cartilage was fixed | Increase in MCS of 44% and increase in CP of 50% after partial lateral meniscectomy | ||
| Pena et al. [52] | 006 | Lateral and Medial meniscectomy | 1150 N, full extension, constrained varus-valgus and flexion-extension rotations of the femur, fixed lower surface of tibia | Increase in maximum shear stress of 98% and 177% after partial and total medial meniscectomies, respectively, Increase in maximum shear stress of 415% and 687% after partial and total lateral meniscectomies, respectively | ||
| Mononen et al. [4] | 2013 | Radial Tear (66%) in LM | Gait cycle data was applied on the reference point, and the bottom surface of tibial cartilage was fixed | Increase in MCS of 44% and increase in CP of 50% after partial lateral meniscectomy | ||
- Pena et al. [47] reported that MCS (FEA) in the tibial cartilage increases by 302% after total medial meniscectomy. This is comparable with the experimental results (136-235%) [26, 28].
- FEA studies found a decrease in CA of 26-45% after total medial meniscectomy [47, 53], which is comparable with the experimental findings (36-80%) [18, 26-28, 35-38].
- Dong et al. [49] found that there was a 43% increase in MCS in tibial cartilage after ~30% partial longitudinal meniscectomy whereas the experimental study by Baratz, Fu, & Mangat [26] reported an increase of 65% after 33% partial longitudinal meniscectomy. Dong et al. [60] considered a load of 1150 N, whereas Baratz, Fu, & Mangat [26] adopted a load of 1800 N. Moreover, menisci and cartilages were treated as elastic instead of viscoelastic. This could be the reason for the discrepancy in the results.
It could be observed that most of the findings of FEA are comparable with the results of experimental studies and the reasons for the disparity in some of the results are discussed with suitable justifications. This confirms the efficacy of FEA in assessing the biomechanical behavior of meniscectomised subjects.
CONCLUSION
This paper provides a combined review of experimental and FEA studies that have been undertaken to investigate the consequences of medial and lateral meniscectomies on the biomechanical parameters of the knee joint. Experimental studies reveal that total medial meniscectomy causes a decrease in CA of 36-80% associated with a substantial increase in the contact stress of 136-235% in comparison with that in an intact knee joint. Whereas the FEA study demonstrates a corresponding decrease in CA of 26% associated with a dramatic increase in the contact stress of 302%. In addition, it leads to extreme degenerative changes in the cartilage.
FEA studies manifest that subtotal medial meniscectomy causes a mean increase in CP of 20-22%, the mean reduction in CA of 18-28% in the cartilage and the mean rise in CP on MM of 70-82% relative to that in an intact knee. FEA studies indicate that partial medial meniscectomy results in an increase in the CP of 14% and reduction in CA of 6% in comparison with that in an intact knee joint. Hence, partial medial meniscectomy is preferable over subtotal/ total medial meniscectomy since it minimizes the degeneration of the cartilage. FEA studies also predict that total lateral meniscectomy results in a remarkable rise (677%) in maximum shear stress in the cartilage compared with medial meniscectomy (177%). This could be the reason for lateral meniscectomy to be more detrimental than medial meniscectomy. Experimental studies show that the resection of both leaflets of the meniscus leads to a significant increase in CP and considerable reduction in CA compared with inferior leaflet resection. Hence, it is suggested to carry out resection of inferior leaflet instead of resection of both leaflets. The FEA technique can be extensively used to determine the consequences of meniscectomy by simulating the meniscectomy condition before performing it in-vivo. The results of FEA studies are compared with those of experimental studies and the reason for the observed difference is discussed with suitable justifications. The results of this study could guide surgeons in deciding the effective meniscectomy protocol to minimize cartilage damage in patients with meniscal injuries.
FUTURE RECOMMENDATIONS
Most of the experimental investigations were performed on cadaveric specimens, which lack the dynamic characteristics of an in-vivo model. Hence, future research should focus on approaches to preserve the dynamic characteristics of the soft tissues. The meniscus is known to be subjected to extreme stresses during sports such as football, soccer and basketball which involve pivoting movements. Hence, future studies have to be performed taking into account the loading conditions corresponding to such activities to investigate the effects of meniscectomies on knee biomechanics.
The FEA studies reported in the literature have considered a smaller sample size. This may be because of the considerable amount of time required to construct the FE model of the knee joint. Since smaller sample size is used, it is not possible to achieve the statistical significance of results leading to difficulty in generalizing the results. Hence, it is recommended to consider a larger sample size to demonstrate statistical significance. Furthermore, the FEA studies have taken material properties from published literature. Hence, future studies have to be carried out by considering subject-specific material properties to predict the realistic biomechanical behavior of the knee joint. In addition, most of the FEA studies reported in the literature have determined the biomechanical parameters by subjecting the knee joint to an axial compressive load. Hence, further research should be carried out by considering the combination of axial, anterior and posterior loads and rotational moments that may occur during in-vivo conditions. Finally, the FEA studies have been performed by simulation of meniscectomy in a healthy subject by the removal of a particular portion of the meniscus in the 3D model. Therefore, future research must take into account the actual meniscectomised subjects to predict realistic biomechanical behaviour.
DISCLOSURES
Part of this article has previously been published in Experimental and Finite Element Investigations on the Biomechanical Effects of Meniscal Tears in the Knee Joint: A Review, in Journal of Biomimetics, Biomaterials and Biomedical Engineering, c, vol 50, pp 1-1.
LIST OF ABBREVIATIONS
| CA | = Contact Area |
| CP | = Contact Pressure |
| FEA | = Finite Element Analysis |
| FE | = Finite Element |
| HCT | = Horizontal Cleavage Tears |
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

