All published articles of this journal are available on ScienceDirect.

An Updated Review on the Impact of an Eye-controlled Wheelchair on Quality of Life of Patients with Neurological Disorders and their Caregivers
Authors Info & Affiliations
Abstract
Background
Paralyzed individuals, depending on their severity, are usually incapable of operating an electric wheelchair because it requires a common method of maneuvering, such as a joystick with buttons to control the chair. In such a case, an eye-controlled wheelchair can be utilized as it functions to facilitate mobility assistance for paralyzed or elderly individuals with limited movement within their natural environment.
Objective
This study aimed to explore the impact of using an eye-controlled wheelchair in a home-care environment on the quality of life of patients with neurological disorders.
Method
This case study was conducted by two neurological condition patients from a local home-care setting. To achieve the research objective, online questionnaires via Google Form were administered verbally after the eye-controlled wheelchair usage and subjects’ feedback was filled by the researchers. The efficiency of using the eye-controlled wheelchair was measured by the subject’s exhaustion level and workload. The total workload needed for wheelchair usage was measured using the National Aeronautics and Space Administration Task Load Index (NASA-TLX) tool, and a self-designed questionnaire was developed and validated (face and content validation) before the commencement of the study to measure subjective quality of life.
Results
The relationship between the quality of life and the total subjective workload was calculated using the Pearson correlation coefficient. Subject A displays a strong positive correlation (r =0.8476, n =8, P<.05), while, for Subject B (r =0.6196, n =8, P>.05), a moderate positive correlation was found between total subjective workload and quality of life. Overall, a positive correlation was observed between subjective workload and quality of life: as the workload decreased through the use of the eye-controlled wheelchair, the quality of life for both patients and caregivers significantly improved.
Conclusion
This study concluded that an eye-controlled wheelchair has a positive impact on the quality of life of patients with neurological disorder. This wheelchair will be beneficial for individuals with limited hand strength who are unable to operate a manual wheelchair or an electric one that uses a joystick or buttons.
1. INTRODUCTION
Cost-effectiveness has led to the widespread use of manual wheelchairs in many Malaysian elderly home-care settings. However, a high occupant-to-carer ratio limits the ability of wheelchair users to move independently within the facility. This challenge particularly affects individuals with limited or no upper limb strength, which is essential for independently operating a manual wheelchair.
A recent study highlights this issue. Although manual wheelchairs offer many benefits, some users do not have the upper body strength necessary for self-propulsion. In such cases, powered wheelchairs are typically recommended. However, individuals with severe physical disabilities may be unable to operate these devices independently, necessitating caregiver’s assistance. Although pushing a wheelchair may appear simple, caregivers often encounter challenges similar to those faced by wheelchair users when moving through physical space. Additionally, prolonged wheelchair pushing can cause fatigue and increase the risk of injury. Products designed to reduce the strain of wheelchair pushing could improve the well-being of both caregivers and users [1]. An eye-controlled wheelchair presents an alternative in such scenarios, with a powered wheelchair serving as the base.
Powered wheelchairs, equipped with electric motors, are usually controlled with joysticks. However, when users cannot coordinate or use their hands or fingers, alternative input methods—such as button control, head control, breath control, or speech control—can be employed [2]. Although powered wheelchairs eliminate most of the physical effort required by manual wheelchairs, they still demand an upright posture and some degree of upper-body mobility for steering [3].
While powered wheelchairs enhance mobility, their benefits diminish as users' upper limb strength deteriorates. Consequently, alternative control methods, such as eye-controlled systems, become necessary. In this study, a powered wheelchair was modified with an eye-tracker, transforming it into an eye-controlled wheelchair. This innovation enables users to control and navigate the wheelchair using eye movements, even if they have lost hand muscle function.
A lower workload has been associated with an improved quality of life (QoL). A study investigating the relationship between workload and job stress among nurses at Vasei Hospital in Iran found a significant inverse relationship between workload and QoL [4]. Similar findings have been reported in other studies, which also indicate that a lower workload leads to a higher QoL among healthcare workers [5, 6]. Reducing caregivers' workload not only alleviates their burden but also enhances the QoL of patients, particularly those with stroke, spinal cord injury (SCI), or poor upper limb strength who struggle to use both manual and powered wheelchairs effectively.
However, to our knowledge, no study has measured QoL among eye-controlled wheelchair users in a home-care environment. Existing studies have focused solely on manual or powered wheelchair users without addressing efficiency-related issues [7-9]. The only efficiency-related study examined workload and exhaustion levels in users of brain-computer interface applications, such as brain-painting [10, 11]. This study adapts similar efficiency measures while incorporating wheelchair usage.
Hence, the present study aims to explore the impact of using an eye-controlled wheelchair in a home-care environment on the QoL of patients with neurological disorders. The specific objectives are:
(a) To evaluate the QoL of the subjects after short-term use of the eye-controlled wheelchair.
(b) To investigate the efficiency of the subjects in using the eye-controlled wheelchair.
(c) To examine the association between subjective workload and QoL.
A previous study examined the efficiency and quality-of-life aspects of using an eye-controlled wheelchair. While our current study builds upon that foundation, it introduces several key methodological and analytical advancements that distinguish it from prior work [12]. One notable addition is the inclusion of comprehensive participant information, ensuring clarity regarding their background before engaging with the eye-controlled wheelchair. This level of detail was not explicitly presented in our previous publication and is essential for understanding the user context and study outcomes.
Furthermore, we have incorporated additional measurement tools to enhance the methodological rigor of our research. Specifically, we assess the efficiency and wheelchair usage through multiple parameters, including exhaustion level, workload, wheelchair usage frequency, number of sessions, time in minutes, and distance in meters. These elements were not included in our earlier work, and their inclusion provides a more comprehensive evaluation of the system’s usability and effectiveness. In addition, to better understand cognitive and physical workload, we have integrated the NASA Task Load Index (NASA-TLX) as an outcome measure, with detailed results presented in Section 3.3.2 Workload. This tool allows for a more structured assessment of the demands placed on users, offering insights beyond what was previously reported.
Moreover, the discussion section has been significantly expanded to provide deeper insights and interpretations of the findings, contextualizing them within the broader research landscape. This comprehensive discussion goes beyond the scope of our prior study and reinforces the novel contributions of this research. By explicitly referencing our previous publication, we clarify that while this study aligns with similar research objectives, its additional methodological components and analytical depth establish its originality and further development in the field.
2. MATERIALS AND METHODS
2.1. Participants
In this qualitative design study, two female geriatric subjects with neurological disorders were recruited from Rumah Seri Kenangan Cheras, a government old folks’ home under the Department of Social Welfare Malaysia after obtaining ethical approval and informed consent. The inclusion criteria required mentally stable, wheelchair-bound individuals with no prior experience using eye-controlled or brain-computer interface wheelchairs, with additional information gathered from medical reports and interviews.
2.1.1. Participants’ Information
Subject A is a 64-year-old female patient with an endomorphic (obese) build who has been residing in the home-care centre for the past five years. Her past medical history includes right breast cancer, for which she underwent a mastectomy in 2017. Additionally, she has been living with diabetes mellitus, hypertension, and dyslipidaemia for the past 10 years and is on medication. Initially, she was able to walk independently; however, three years ago, she suffered a fall while bathing, resulting in an injury to her lumbar region and a left femoral neck fracture.
Her recent spinal cord injury is linked to a past injury at the lumbar region (L4) sustained during a school hockey match, which led to a hairline fracture. As a result, she developed an L1 spinal cord injury, leading to paraplegia and confinement to a manual wheelchair for mobility. As she ages and her health declines, she has experienced significant upper limb muscle weakness. Currently, she relies on both her manual wheelchair and a caregiver to assist her in moving from her room to other locations within the facility, depending on her needs and preferences.
Examples of scenarios where Subject A requires mobility assistance include:
- Attending spiritual talks organized by the home-care center at the Surau1 within the compound.
- Meeting and chatting with friends from different clusters or dorms.
- Taking a walk after prolonged periods of lying down or watching television in her room.
- Visiting the in-house clinic to consult with nurses and collect medications.
Subject A further expressed that, at times, she chooses to remain in bed rather than attend events at the Surau or socialize with her friends due to the unavailability of caregivers, who are often occupied with assisting other residents.
Her primary concern can be summarized as participation limitation, leading to a reduced QoL— specifically in terms of independence and social interaction. Despite her health challenges, she is sociable, enjoys engaging in conversation, and has a good sense of humour.
Subject B is a 75-year-old female patient with an endomorphic (obese) build who has been residing in the home-care centre for the past seven years. She was diagnosed with atypical T-cell lymphocytes in 2013 and completed radiotherapy. Since 2009, she has also been living with diabetes mellitus and hypertension, for which she is on medication.
Due to her age and weight, she developed bilateral knee osteoarthritis (Stage 2) in 2010. In 2011, she suffered an ischemic stroke, which resulted in paraplegia. Additionally, aging and declining health have led to poor upper limb muscle strength, further limiting her mobility. Since then, she has been dependent on a manual wheelchair.
Despite her condition, Subject B remains cheerful and enjoys eating, talking, and meeting people. Her hobbies include attending talks or gatherings organized by the home-care center and socializing with friends. She currently relies on both her manual wheelchair and a caregiver for mobility assistance.
Examples of scenarios where Subject B requires mobility assistance include:
(1) Attending talks organized by the home-care centre.
(2) Meeting and chatting with friends from different dorms.
(3) Taking a walk after socializing with her roommates.
(4) Visiting the in-house clinic to consult with nurses and collect medications.
She further mentioned that, at times, she remains in her room rather than attending events at the main hall or visiting her friends' rooms due to caregivers being occupied with assisting other residents (e.g., bathing or feeding them). Unlike Subject A, she does not engage in specific hobbies but enjoys chatting with friends by the window and watching television, regardless of the program being aired.
Similar to Subject A, Subject B’s primary concern is participation limitation, leading to a reduced QoL—particularly in terms of independence and social interaction.
2.2. Procedure
The experiment began with the subject seated in a wheelchair. The eye tracker was fixed to the laptop, and the screen of the wheelchair system was positioned within a range of 30–50 cm from the subject’s eye level.
At the beginning of each session, verbal instructions were provided on the procedure for navigating and controlling the eye-controlled wheelchair. During this instruction phase, subjects were encouraged to ask questions or express any concerns regarding the wheelchair's operation. All queries raised were addressed accordingly, and verbal confirmation of consent to participate in the study was obtained once again.
1The Surau is an Islamic worship place similar to a mosque but with a smaller structure.
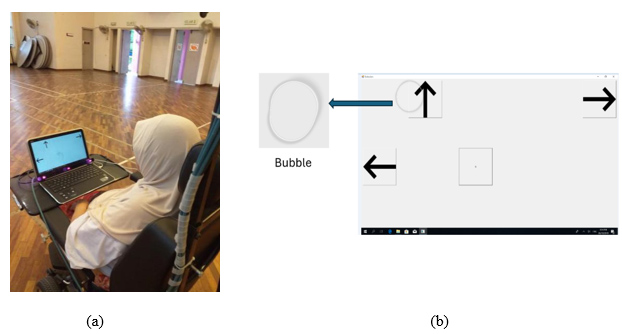
(a) Subject is looking at the selection box on the laptop screen to select her desired direction. She is navigating and controlling the wheelchair with the aid of the eye-tracker device [12]. (b) Reflection of subject’s eye gaze as ‘bubble’ which ease their selections. The bubble represents the point the subject is looking at the selection screen.
A few trial sessions were conducted to familiarize the subjects with the system. After the trial sessions were completed, the subjects were allowed to independently control and navigate the eye-controlled wheelchair with minimal supervision from the researcher. This approach ensured that the researcher’s presence did not introduce any bias in the outcome measures. The duration of wheelchair navigation was entirely based on the subject’s willingness to move around. Each subject attempted a minimum of three sessions per week.
Subjects were instructed to select their desired direction by looking at a designated box displayed on the laptop screen (Fig. 1). Each box represented a specific direction—forward, right turn, left turn, or stop—facilitating navigation through eye control.
A preliminary test run was conducted before the study to assess the wheelchair's speed and make necessary visual screen modifications [11].
2.3. Efficiency Measure
The operational definition of efficiency in this study is based on the subject’s exhaustion level and workload in addition to data associated with wheelchair usage. The subject’s workload assessment was standardized to every Monday of the week, while wheelchair usage was recorded after each session [10].
Exhaustion level and workload are subjective measurement tools, as the data are collected from the subjects' self-reports. In contrast, wheelchair usage is an objective measurement tool, as the data are obtained through researcher observation and measurement, without incorporating the subjects' perspectives.
2.3.1. Usage of the Wheelchair
The usage of the eye-controlled wheelchair was measured based on the number of sessions completed, session duration, and distance travelled. The distance was calculated from the wheelchair’s start to the endpoint using a BOSCH GLM 40 laser range finder, with both points marked by neon-coloured stickers. A designated box at the start point served as a laser barrier to ensure consistent measurement. The researcher, standing at the endpoint, aimed the laser at the box, and the displayed value was recorded in Google Sheets. Stickers were removed after each measurement to prevent errors, with distances measured at both the start and end of each session.
Session duration was recorded using a smartphone stopwatch from the start to the end of each session, with the results saved directly in Google Sheets. All collected data, including subject responses, were automatically stored in Google Drive through Google Forms and Sheets.
2.3.2. Exhaustion Level
Exhaustion level refers to physical, mental, or combined fatigue [13]. While the Borg Rating of Perceived Exertion and the Fatigue Severity Scale assess physical exertion, they were deemed unsuitable for this study, as they focus on general physical work rather than wheelchair-related fatigue [14, 15].
Instead, subjects rated their exhaustion levels as high, medium, or low through verbal feedback at the end of each session. The researcher recorded their responses by selecting the corresponding answer in a pre-set Google Form via a smartphone.
2.3.3. Workload
The subject’s workload was measured using the NASA Task Load Index (NASA-TLX), which defines workload as the effort required to achieve a certain performance level across six domains: mental demand, effort, frustration, performance, temporal demand, and physical demand [16]. Subjects rated these domains on a scale from 0 to 100, and their verbal responses were recorded in a pre-set Google Form via the researcher’s smartphone.
An online NASA-TLX tool (2019) was used to calculate the total workload score (0–100) and determine the contribution of each domain.
2.4. QoL
The Quality of Life Related to Wheelchair (QOLRW) questionnaire consists of 16 items across five domains:
- General feeling (4 items)
- Self-esteem (2 items)
- Social interaction/independence (2 items)
- User-friendliness (4 items)
- General health (4 items)
It uses a 5-point Likert scale ranging from -2 (Strongly Disagree) to 2 (Strongly Agree) and takes approximately 15 minutes to complete. A Visual Analog Scale with facial reactions was included to assist in scoring. The total score (maximum 32) and individual domain scores provide insights into the subjects' QoL. The overall QoL was categorized as better, unchanged, or worse compared to the beginning of the sessions.
2.4.1. Questionnaire Administration
The data collection frequency was adjusted from once a week to once a month while QoL data continued to be collected weekly. The researcher read the questionnaire aloud to the subjects and recorded their verbal responses in a pre-set Google Form on a smartphone, with the data automatically stored in Google Drive [10].
2.5. Data Analysis
The first objective is to assess the subjects' QoL after short-term use of the eye-controlled wheelchair. QoL scores will be analysed using descriptive statistics.
The second objective is to evaluate the efficiency of wheelchair use, which includes:
- Wheelchair usage – measured by the number of sessions, duration (minutes), and distance travelled (meters).
- Exhaustion levels – as reported by the subjects.
- Workload scores – to assess subjective workload.
These parameters will also be analysed using descriptive statistics.
The third objective is to explore the relationship between workload and QoL. The Shapiro-Wilk test will be used to check for normality, followed by Pearson’s correlation coefficient, to determine the association between workload and QoL scores.
3. RESULTS
3.1. Quality of Life Score
The QoL was measured using the self-designed QOLRW questionnaire. Table 1 shows a progressive increase in subjects' QoL throughout the study, indicating a positive impact of wheelchair navigation across all domains: general feeling, self-esteem, social interaction/ independence, user-friendliness, and general health. Both subjects showed improved QoL compared to their fourth- and eighth-week assessments.
Subject A consistently rated most items as “agree” or “strongly agree” across all domains. Similarly, Subject B provided comparable ratings during the first assessment.
| Subject | Domain | Week 4 | Week 8 | Score | Total Score by Domain2 | *Improvement in each Domain (%) | Effect Size** |
|---|---|---|---|---|---|---|---|
| Score | Score | Difference1 | |||||
| A | General Feeling | 5 | 7 | 2 | 8 | 25 | Small |
| Self-esteem | 2 | 4 | 2 | 4 | 50 | Small | |
| Social Interaction/Independence | 2 | 4 | 2 | 4 | 50 | Small | |
| User-friendly | 7 | 7 | 0 | 8 | 0 | N/A | |
| General Health | 5 | 8 | 3 | 8 | 38 | Small | |
| Total Score | 21 | 30 | 9 | 32 | - | - | |
| B | General Feeling | 4 | 6 | 2 | 8 | 25 | Small |
| Self-esteem | 2 | 4 | 2 | 4 | 50 | Small | |
| Social Interaction/Independence | 2 | 4 | 2 | 4 | 50 | Small | |
| User-friendly | 7 | 8 | 1 | 8 | 13 | Small | |
| General Health | 7 | 7 | 0 | 8 | 0 | N/A | |
| Total Score | 22 | 29 | 7 | 32 | - | - |
3.2. Progress Summary
By the fourth week, Subject A scored 21/32, and Subject B scored 22/32, showing comparable initial QoL. In the eighth week, Subject A scored 30/32, and Subject B scored 29/32, reflecting noticeable improvements: a 9-point increase for Subject A and a 7-point increase for Subject B.
Score Changes by Domain (Week 8 - Week 4):
- Subject A: General feeling (+2), Self-esteem (+2), Social interaction/independence (+2), User-friendliness (+0), General health (+3)
- Subject B: General feeling (+2), Self-esteem (+2), Social interaction/independence (+2), User-friendliness (+1), General health (+0)
The total score improvements across both subjects by domain were: General feeling (+8), Self-esteem (+4), Social interaction/independence (+4), User-friendliness (+8), and General health (+8).
The improvement of the score in each domain (%) was calculated using this formula (1):
 |
(1) |
The improvement in each domain (%) was calculated using the formula below to compare QoL score changes between weeks 4 and 8:
- Subject A: General feeling (25%), Self-esteem (50%), Social interaction/independence (50%), User-friendliness (0%), General health (38%)
- Subject B: General feeling (25%), Self-esteem (50%), Social interaction/independence (50%), User-friendliness (13%), General health (0%)
Effect size, which measures the strength of the relationship between variables [17], was calculated for each domain:
- Subject A: A small effect size was observed across general feeling, self-esteem, social interaction /independence, and general health, while user-friendliness had no measurable effect size.
- Subject B: A small effect size was found for general feeling, self-esteem, social interaction/independence, and user-friendliness, with no effect size for general health.
3.3. Efficiency Measures
The study aims to assess the efficiency of the subjects in using the eye-controlled wheelchair. Efficiency was measured by wheelchair usage (session, duration, and distance), exhaustion level, and workload.
3.3.1. Wheelchair Usage
The data on wheelchair usage is presented in Table 2. Subject A completed 32 sessions and Subject B completed 29, with each session corresponding to one day. In total, both subjects completed 61 sessions. Subject A spent 1,722 minutes traveling 5,207 meters, while Subject B spent 1,492 minutes traveling 2,687 meters.
Subject A travelled 5,207 meters over 32 days (32 sessions), while Subject B covered 2,687 meters over 29 days (29 sessions).
3.3.2. Workload
The subjects' workload, assessed using the NASA Task Load Index, is summarized in Table 3. The six workload domains measured were mental demand, effort, frustration, performance, temporal demand, and physical demand.
| Subject | Total Sessions Completed (n) | Total Duration Spent (min) | Total Distance Travelled (m) |
|---|---|---|---|
| A | 32 | 1,722 | 5,207 |
| B | 29 | 1,492 | 2,687 |
| Week of study | ||||||||||
| Subject | Dimension | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Mean |
| A | Mental demand | 2.67 | 5.00 | 3.67 | 3.73 | 2.67 | 1.33 | 2.00 | 0.67 | 2.72 |
| Physical demand | 0.00 | 0.33 | 0.80 | 1.00 | 0.33 | 0.67 | 0.67 | 0.13 | 0.49 | |
| Temporal demand | 1.33 | 0.33 | 0.27 | 0.27 | 0.67 | 0.67 | 0.33 | 0.13 | 0.50 | |
| Performance | 9.20 | 10.93 | 10.67 | 10.13 | 8.67 | 5.60 | 8.33 | 1.87 | 8.18 | |
| Effort | 16.8 | 14.80 | 8.40 | 3.40 | 4.00 | 6.67 | 5.07 | 4.67 | 7.98 | |
| Frustration | 0.33 | 0.33 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.08 | |
| - | Total workload | 30.33 | 31.72 | 23.81 | 18.53 | 16.34 | 14.94 | 16.40 | 7.47 | 19.94 |
| B | Mental demand | 1.73 | 2.40 | 1.33 | 1.00 | 1.00 | 0.80 | 0.53 | 0.40 | 1.15 |
| Physical demand | 17.40 | 0.93 | 0.53 | 0.67 | 0.27 | 1.07 | 0.80 | 0.80 | 2.81 | |
| Temporal demand | 0.53 | 0.33 | 0.67 | 0.67 | 1.00 | 0.27 | 1.00 | 0.60 | 0.63 | |
| Performance | 19.00 | 4.27 | 3.00 | 4.00 | 3.33 | 2.80 | 1.20 | 1.00 | 4.83 | |
| Effort | 1.67 | 2.33 | 1.33 | 1.33 | 0.80 | 1.07 | 1.33 | 0.80 | 1.33 | |
| Frustration | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | |
| - | Total workload | 40.33 | 10.26 | 6.86 | 7.67 | 6.40 | 6.01 | 4.86 | 3.60 | 10.75 |
For Subject A, the mean scores were:
- Lowest: Frustration (0.08), Physical demand (0.49), Temporal demand (0.50)
- Moderate: Mental demand (2.72)
- Highest: Effort (7.98), Performance (8.18)
For Subject B, the mean scores were:
- Lowest: Frustration (0.00), Temporal demand (0.63)
- Moderate: Mental demand (1.15), Effort (1.33)
- Highest: Performance (4.83)
Overall, the total workload for both subjects was low:
- Subject A: Mean score = 19.94
- Subject B: Mean score = 10.75
These results suggest that both subjects experienced a relatively low workload across the assessed domains.
3.4. Association between Subjective Workload and QoL
The Shapiro-Wilk test was conducted on the collected subjective workload and QoL data to determine whether they followed a normal distribution. A right-tailed normal distribution was applied, and the results showed that both workload and QoL data for each subject were normally distributed. Since p-value > α, we failed to reject the null hypothesis (H0), indicating no significant difference between the data sample and a normal distribution.
A Pearson correlation was computed to assess the relationship between subjective workload and QoL for each subject:
- Subject A: Strong positive correlation (r = 0.8476, n = 8, p < 0.05)
- Subject B: Moderate positive correlation (r = 0.6196, n = 8, p > 0.05)
Overall, a positive correlation was found between workload and QoL, indicating that QoL increases as workload decreases.
4. DISCUSSION
The growing elderly population requires greater investment in assistive technologies to enhance mobility and improve QoL [18]. This study focuses on two elderly patients with neurological disorders and upper limb muscle weakness, identifying them as potential users of the eye-controlled wheelchair. As their health deteriorates due to aging and disease progression, the wheelchair offers significant benefits.
The wheelchair is particularly useful for individuals with upper limb muscle weakness, though its implementation in conditions like ALS may be challenging.
4.1. Quality of Life (QoL)
The QoL impact of the eye-controlled wheelchair was measured using the QOLRW questionnaire. To minimize bias, the researcher accompanied each subject for only five sessions to foster trust and confidence. Both subjects were former manual wheelchair users with no prior experience using powered or eye-controlled wheelchairs.
This study highlights that functional limitations due to neurological impairments affect activities of daily living (ADLs), including bathing, dressing, and walking [19, 20]. Reduced outdoor activities can limit social participation, increasing the risk of depression.
Both subjects were assisted by caregivers for ADLs, including bathing, dressing, and wheeling between locations. While both had minimal hand function, their conditions limited the long-term use of standard powered wheelchairs due to morbidity, co-morbidity, and age-related decline [21, 22].
Despite these challenges, both subjects enjoyed social interaction and moving around their care home but often depended on others for mobility, reducing their independence and QoL. The eye-controlled wheelchair improved their sense of freedom and social interaction, as reflected in the QOLRW domains: self-esteem, independence, social interaction, user-friendliness, and general health. However, it had a slightly negative impact on general feelings, as both subjects initially struggled to adapt to the system.
Previous studies on assistive technologies, such as brain-controlled systems, have demonstrated QoL improvements for patients with neurological conditions [10, 23]. Other studies have used standardized QoL questionnaires like the World Health Organization Quality of Life - BREF, European Quality of Life - 5 Dimensions, and Short Form (36) Health Survey to assess the impact of wheelchairs on QoL [7-9].
This study is among the first to explore QoL using eye-controlled wheelchairs in home-care settings. The QOLRW questionnaire, with its visual analog scale and emoji-based responses, made it easier for subjects to provide feedback and navigate the system with minimal effort.
4.2. Efficiency Measures
4.2.1. Wheelchair Usage
The wheelchair usage was measured by the number of sessions, duration per session, and distance travelled.
- Subject A: 32 sessions, 1,722 minutes, 5,207 meters
- Subject B: 29 sessions, 1,492 minutes, 2,687 meters
Variations in distance and session durations were attributed to the subjects' declining health. However, both subjects remained enthusiastic, describing the wheelchair as “fun, new, and interesting.” The design allowed them to navigate freely without strict targets, aligning with studies that measure assistive device usage in terms of sessions, duration, and distance [24, 25].
4.2.2. Exhaustion Level
Exhaustion was rated on a three-point scale (low, medium, or high) based on verbal feedback from the subjects after each session. This approach mirrored a similar rating system used in a brain-controlled painting application study for ALS patients [10].
- Subject A: Reported 4 high-exhaustion sessions, with the remaining sessions rated as low or medium.
- Subject B: Reported 9 medium-exhaustion sessions, with the rest rated as low.
The ease of navigation using the eye-tracker device contributed to the overall low exhaustion levels.
Across 61 sessions, both subjects mostly reported low exhaustion (Fig. 2):
- Subject A: Initially found the first 4 sessions highly exhausting but progressed to a lower exhaustion level over time.
- Subject B: Rated the first 9 sessions as medium exhaustion but later reported low exhaustion.
4.2.3. Workload
The NASA-TLX defines workload as “a hypothetical construct representing the cost incurred by a human operator to achieve a particular level of performance” [16, p.140]. Its main domains include mental, physical, and temporal demands, along with performance, effort, and frustration levels. In this study, NASA-TLX measured subjective workload after using the eye-controlled wheelchair.
Subject A reported a mean workload score of 19.94, while Subject B scored 10.75. For Subject A, performance (mean = 8.18) and effort (mean = 7.98) were the primary sources of workload, whereas Subject B experienced a higher physical demand (mean = 4.83) and performance pressure (mean = 1.33). Both participants identified as perfectionists, frequently adjusting the wheelchair until it reached their desired position. This suggests that their workload was influenced by personal goals rather than system limitations.
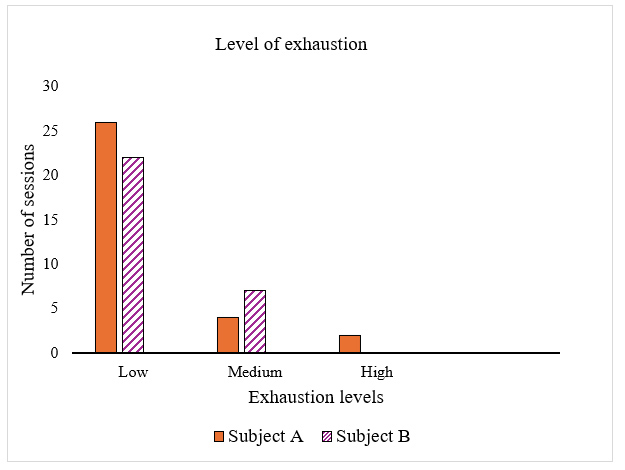
Subject’s exhaustion level.
The low workload scores indicate that the wheelchair's user-friendly design contributed significantly to ease of use. Both participants noted that the wheelchair was easy to control and navigate with the aid of the eye-tracker. The system’s “bubble” feature, which provides on-screen visual feedback, enabled them to select directions by focusing and blinking. Notably, Subject A, a spectacle wearer, reported smooth performance, demonstrating the device's effectiveness for users with visual aids. The low workload and minimal exhaustion motivated both participants to engage regularly with the wheelchair.
Previous studies also support the effectiveness of assistive wheelchair technologies:
- A study found that participants experienced a low workload while using an Intelligent Wheelchair System [26].
- A study reported low NASA-TLX scores during trials with virtual reality-powered wheelchairs [27].
- Recent research observed that users with tetraplegia experienced low-to-medium workload using a myoelectric control system [28].
- However, another study noted that a mobility-enhancement robotic wheelchair induced a higher mental workload due to its complexity [29].
4.3. Subjective Workload and QoL
This study explored the relationship between subjective workload and QoL, finding a positive correlation whereby QoL improved as workload decreased. The wheelchair’s ease of use and user-centered design likely contributed to this outcome.
Research suggests that individuals who depend on manual wheelchairs may benefit from powered alternatives [30]. While manual wheelchairs provide mobility benefits, some users lack the upper body strength to propel themselves and often rely on caregivers. However, caregivers also face challenges such as fatigue and strain from prolonged wheelchair use, which can negatively affect both users and caregivers [1]. Eye-controlled wheelchairs could be an effective alternative, reducing physical burden and caregiver involvement.
Consistent with the study hypothesis, a lower workload was associated with improved QoL. A study [10] also found similar improvements with powered wheelchair use. While this study confirmed the workload-QoL relationship, further research is needed to explore this association more extensively in wheelchair users.
4.4. QoL Measurement in Stroke and SCI Patients
Reduced mobility often leads to diminished QoL in stroke and SCI patients [8, 9]. A cross-sectional study by Hosseini et al. found that better manual wheelchair skills predicted a higher QoL among 214 SCI patients. However, previous studies have primarily focused on manual or powered wheelchairs, whereas this study explored QoL outcomes with an eye-controlled wheelchair [7].
Stroke is a leading cause of disability worldwide [31]. Patients often rely on informal caregivers, such as family members, during and after rehabilitation [32]. Caregiving responsibilities can become burdensome, affecting caregivers' mental health [33]. Research shows that patient recovery positively impacts caregiver QoL [34].
4.5. Comparison with Other Assistive Devices
The eye-controlled wheelchair (ECW) can be compared to other assistive wheelchairs, such as brain-signal-controlled, tongue-controlled, speech-controlled, head-movement-controlled, and electrically joystick-operated wheelchairs [35].
Joystick-operated wheelchairs pose limitations for patients who lack upper limb mobility or dexterity due to conditions affecting the hands and shoulders. Patients with increased muscle tone or rigidity may experience reduced movement control and finger strength, making joystick operation difficult. Additionally, limited head movement may increase the risk of collisions or falls from the wheelchair. Age is another factor, as older adults generally exhibit lower hand dexterity compared to younger adults [36].
Brain-signal-controlled wheelchairs using brain-computer interface technology offer a real-time interface via an electroencephalography headset, providing a non-invasive option. However, several limitations exist:
- The user’s mental state must remain stable throughout the wheelchair operation.
- Cognitive ability and training are required to operate the wheelchair in various environments.
- High cost remains a major barrier [37].
Tongue-controlled wheelchairs, which use a magnet attached to the tongue, also have potential risks, such as the magnet falling off after a few hours or accidental aspiration of the loose magnet [38].
The ECW overcomes many of these limitations by bypassing the need for upper limb mobility, dexterity, tongue movement, or speech, providing a gaze-based control system that ensures more stable command input than brain-controlled wheelchairs, which may be affected by unstable mental states [39].
However, ECWs also have drawbacks:
- The infrared light used to track eye movement may cause irreversible eye damage or eye strain with prolonged exposure.
- Sensor sensitivity to head movement and lighting conditions can affect system performance [39].
4.6. Reduces Caregiver’s Burden
The ECW impacts caregivers in multiple ways, including reducing caregiver burden, improving patient-caregiver interactions, and introducing new challenges.
4.6.1. Reduced Physical and Emotional Burden
Compared to a non-motorized wheelchair, the ECW enhances patient independence by eliminating the need for upper limb strength to propel the wheelchair. This reduces the physical strain on caregivers who would otherwise assist in pushing a manual wheelchair. Additionally, by minimizing social exclusion, the ECW alleviates caregivers’ emotional burden, as they no longer feel responsible for the patient’s mobility limitations [40].
With the increased autonomy provided by the ECW, patients can move around freely, allowing caregivers more time to focus on other responsibilities rather than physical interventions, such as repositioning the wheelchair.
4.6.2. Improved Patient-Caregiver Interaction
The ECW allows caregivers and users to engage beyond basic mobility, facilitating more complex activities. Instead of focusing on manual assistance, caregivers can strengthen emotional bonds with patients by involving them in ADLs and instrumental activities of daily living. These activities may include grocery shopping, walking in the park, or caring for pets, thereby enhancing the patient's sense of self-worth while reducing caregiver frustration.
Seeing a patient regain independence and take control of his or her own life can be rewarding for caregivers, increasing their job satisfaction.
4.6.3. Challenges for Caregivers
Despite its benefits, the ECW presents new challenges for caregivers. They may still be responsible for operating, maintaining, and troubleshooting the wheelchair system. Older caregivers who are less familiar with computerized interfaces may experience anxiety over software errors or misconfigurations, which could endanger the patient.
Supervision is still required for eye-tracking errors, which could lead to unintended or unsafe movements. In cases of reduced eye endurance or system malfunction, caregivers may need to manually push the wheelchair. To enhance safety, a remote emergency button is available for caregivers, allowing them to assess the situation from a third-person perspective [40]. However, constant vigilance can increase caregivers' alertness and emotional stress.
Additionally, hired caregivers may face job insecurity as automated ECWs reduce the need for direct physical assistance.
4.6.4. Challenges Identified in ECW Research
A study on ECW users with amyotrophic lateral sclerosis (ALS) found that patients were generally satisfied with the independence provided by the device [41]. However, the study highlighted several challenges, including:
- Sunlight interference affects ocular tracking sensors, particularly in outdoor environments or under specific lighting conditions, such as direct sunlight or incandescent bulbs.
- Difficulty with reversing, with one-third of participants requesting a backup camera.
- Challenges for patients with strabismus who struggled to maneuver the ECW.
- Caregiver assistance is still required for vehicle transfers, as patients need help moving from the ECW into a car.
4.6.5. Striving for a Balance between Autonomy and Ethical Concerns
The increasing use of advanced technologies such as ECWs in healthcare raises ethical concerns, particularly regarding privacy, accessibility, and reliance on artificial intelligence for critical mobility functions.
4.6.6. Privacy Concerns
Eye-tracking data is classified as sensitive information, as it contains detailed insights into human attention, emotions, cognitive functions, preferences, and mental states [42]. This poses a significant risk to user privacy, especially if malicious service providers compile large databases to classify personal user data, including identity and gender, and exploit unauthorized data for marketing or surveillance purposes [42].
Another ethical concern involves the objectives of data protection systems. While these systems are designed to protect user data from third parties, privacy breaches occur if the system is used to influence and control users' thoughts and behaviours without their knowledge. Additionally, users may not always be fully aware of how developers, healthcare providers, or businesses collect, store, or use their data. Some systems may collect more data than necessary or use it for unintended purposes.
The balance between user privacy and system utility is entirely controlled by system providers. If this balance is not maintained, utility and profit may be prioritized over privacy, leading to potential exploitation. To mitigate risks, legal requirements should regulate the collection, storage, and use of highly sensitive eye-tracking data. Furthermore, strong cybersecurity measures must be enforced to safeguard user safety [43].
4.6.7. Accessibility and Socio-Economic Barriers
ECWs are expensive and are often inaccessible to individuals from a lower socio-economic group and developing countries. This creates a barrier to equal care and treatment for people with disabilities, particularly those in rural areas who have limited access to assistive technology and necessary medical support.
This lack of accessibility violates the ethical principle of distributive justice, which ensures equal access to healthcare resources for all individuals, regardless of their socio-economic status [44]. To promote fairness, ethical bodies should focus on reducing costs or offering subsidies for these technologies, potentially integrating them into public health programs.
4.6.8. Over-reliance on AI and Loss of Autonomy
Delegating critical healthcare tasks to AI systems may cause users to become overly dependent on technology, potentially reducing their autonomy and favouring machines over human caregivers. This can be particularly dangerous for individuals with cognitive impairments, as they may unknowingly issue hazardous commands to AI-controlled devices, putting themselves at risk.
Another ethical challenge is the loss of interpersonal interactions in healthcare. Replacing human caregivers with technology may lead to reduced trust and understanding, which is a widely debated ethical issue [45, 46].
4.6.9. Safety and Accountability in AI-Driven Systems
Safety is a major ethical concern when AI-powered systems interact directly with the physical world, such as autonomous vehicles, mobility devices like wheelchairs, or systems controlling essential healthcare services. If safety is compromised, determining who is responsible for failures becomes unclear [45]. Establishing clear accountability and ensuring rigorous safety testing are crucial to addressing this issue.
5. LIMITATIONS OF THE STUDY
The primary limitation of this study was the limited availability of participants, as session schedules depended on their health conditions and medical appointments. Despite these challenges, both subjects expressed a willingness to use the eye-controlled wheelchair daily. Over the two-month data collection period, they completed 32 and 29 sessions, respectively.
The nature of the case study design limits the generalizability of the findings to neurological patients. Additionally, the wheelchair was customized for each participant, making it a highly individualized intervention. This study also did not compare the eye-controlled wheelchair with other electric models and only face and content validation of the QoL questionnaire was performed.
As a case study, the findings lack internal validity and cannot establish external validity at this stage.
6. RECOMMENDATIONS FOR FUTURE RESEARCH
Future research should explore the long-term use of eye-controlled wheelchairs in home-care settings to identify potential technical and maintenance challenges. Developers could enhance powered wheelchairs by integrating eye-tracking technology as an alternative to traditional joystick controls.
Additionally, researchers should conduct randomized controlled trials to validate the effectiveness of eye-controlled wheelchairs and further refine the QOLRW tool.
CONCLUSION
This case study explored the impact of eye-controlled wheelchair use on QoL in two geriatric patients with neurological disorders. The wheelchair was implemented in a home-care setting, and participants used it for a total of 3,214 minutes over eight weeks. The study found that its ease of use, aided by features like “Gaze Trace,” contributed to low workload and exhaustion levels. Positive changes in QoL were observed, particularly in general health, independence, and self-esteem.
Findings suggest that even short-term use of an eye-controlled wheelchair can enhance QoL for individuals with neurological disorders.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the manuscript as follows: the study conception and design were carried out by KK and PK; methodology was developed by DWKN; and conceptualization was led by LFT. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| QoL | = Quality of Life |
| ECW | = Eye-Controlled Wheelchair |
| ADL | = Activities of Daily Living |
| SCI | = Spinal Cord Injury |
| NASA-TLX | = National Aeronautics and Space Administration Task Load Index |
| QOLRW | = Quality of Life Related to Wheelchair |
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
This study was supported by the Universiti Tunku Abdul Rahman Scientific and Ethical Review Committee (Ref: U/SERC/99/2018) and the Department of Social Welfare, Malaysia (Ref: JKMM 100/12/5/2: 2018 / 326).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the IEEE Xplore at https://ieeexplore.ieee.org/document/ 9718404, doi: 10.1109/CSDE53843.2021.9718 404.
FUNDING
This work was supported by: Agency: Universiti Tunku Abdul Rahman, Malaysia Funder ID: Universiti Tunku Abdul Rahman Research (Malaysia) Fund 2018 Cycle 2, Grant Number: IPSR/RMC/UTARRF/2018-C2/T01.
ACKNOWLEDGEMENTS
We would like to convey our appreciation to Dato’ Prof. Dr. Goh Sing Yau of Universiti Tunku Abdul Rahman, Malaysia, for his invaluable guidance. We also extend our gratitude to the Department of Social Welfare Malaysia, the research participants, and everyone who contributed to this study, both directly and indirectly.

